

If you haven’t taken a look at the question- please refer to the previous blog post:
If you have read and want to see the answer, please continue reading below…
The patient in last week’s case was found to have an echinococcal liver cyst.
Echinococcus is a tapeworm that exists among carnivorous predators, including dogs and wolves, with intermediate hosts being sheep, goats and cattle. Humans tend to be dead-end hosts, with transmission occurring through the ingestion of eggs, which are found in infected stool. These eggs enter into the intestinal tract of humans, and there, the eggs hatch and penetrate the intestinal lumen in order to enter the bloodstream, from which they can enter into various organs (predominantly the liver and lungs) and produce cysts containing protoscolices, which in turn can produce more eggs. Two primary pathogenic species exists: Echinococcus granulosus, and Echinococcus multilocularis. Diagnosis is aided in part by imaging of the cysts, which often have a unique appearance. Ultrasonography is the imaging modality of choice, and serology testing can help support the diagnosis. Treatment usually consists of antiparasitic therapy in conjunction with surgical intervention/aspiration procedures.
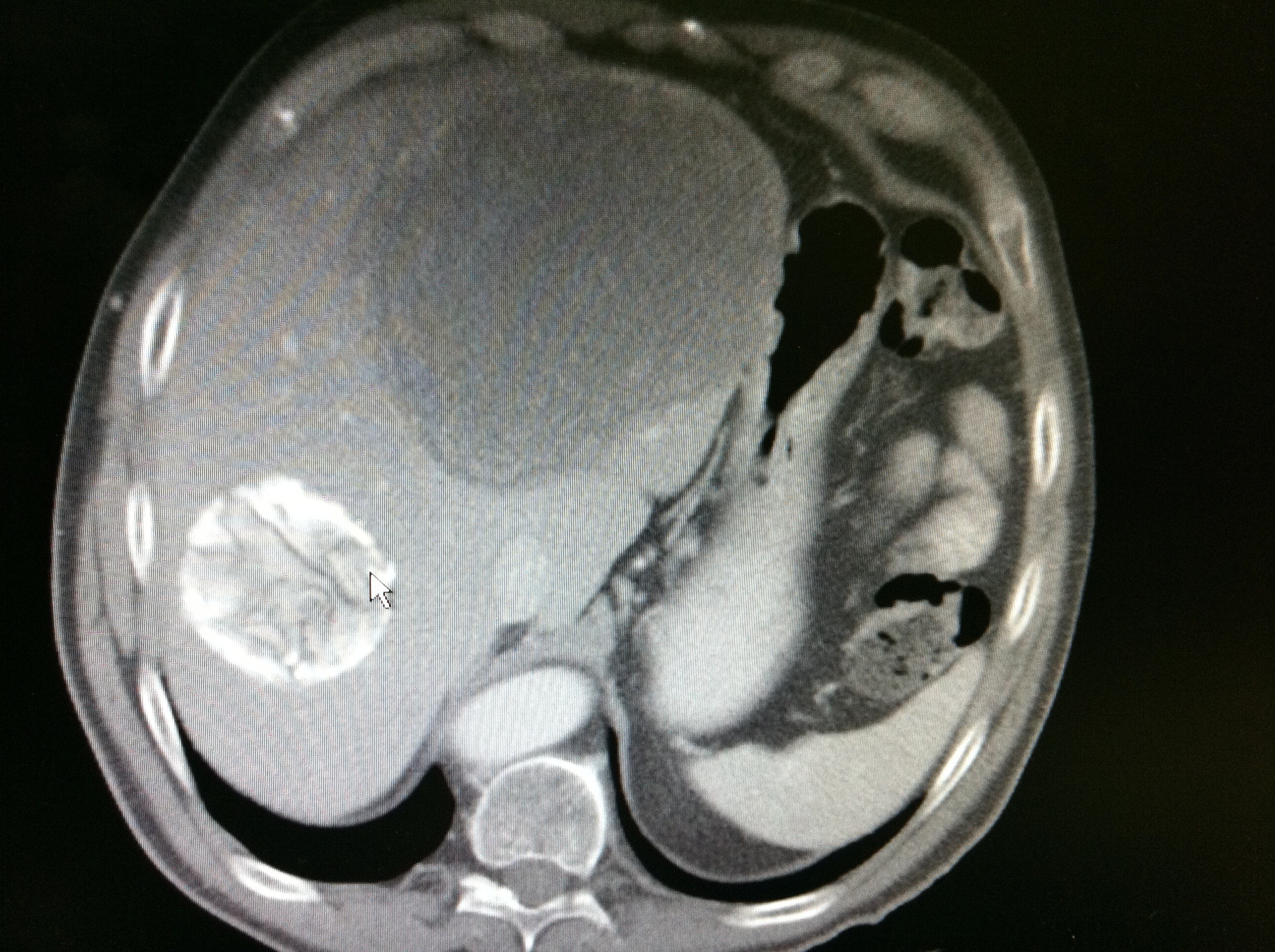
This patient’s history of farming, along with his country of origin (China) are clues associated with echinococcal liver disease, also known as Hyatid Disease. On the CT scan, you can see multicystic liver disease and even part of a scolex (see arrow)
Given the size of his lesion, a PAIR (puncture, aspirate, inject, re-aspirate) procedure was not an option for this patient, and careful surgical removal of the cyst was undertaken as spillage of the cystic contents can predispose patients to anaphylaxis. Surgical drainage, in conjunction with albendazole therapy, resulted in complete resolution of his lesion and symptoms in 6 month’s time.
As to why the other answers are incorrect:
Hepatocellular carcinoma does not produce multi-cystic lesions, and the lesions present are not consistent with an Entamoeba liver abscess, which tends to not be polycystic in nature. Tuberculosis and Q-fever are not associated with cystic liver disease, and Fasciola infection tends to cause biliary obstruction, rashes and hepatomegaly rather than cystic liver disease, and is transmitted by consumption of watercress.
Echinococcus granulosus life cycle from CDC website:


Leave a comment